

What comes to your mind when you hear "Telemedicine"?
One might think that Telemedicine is all about the internet, video calling, and wearable devices, etc., but it's not limited to just those things.
We all know that Telemedicine revealed its real potential amidst the Covid-19 pandemic when it became a necessity, and the medical industry could not proceed without!
Although Telemedicine has become widely popular in recent times, proof of its existence goes back to ancient Greek and Roman civilizations around 500 B.C. It includes Smoke, Fire, and Loud sounds by drums or other means - and were used to signify events such as birth, death, or disease outbreaks.
The more recent incarnation of Telemedicine as we know it now, came in April 1924 in a radio news magazine titled "The Radio Doctor - Maybe!" where it showed patients interacting with doctors via a television like screen and a microphone - it also showed a few ECG graphs getting printed out from the device. The remarkably interesting thing here is that television wasn’t invented in 1927!
Although it was a very wild prediction – it is quite surprising that has taken almost one hundred years for the world to start to leverage Telemedicine to its full potential.
Telemedicine Amidst Covid-19 times
There is little doubt that the Covid pandemic hastened the growth of Telemedicine.
Data shows that use of Telemedicine hiked from 11 % to 76 % from 2019 to 2022.
So, one clear beneficiary of the COVID-19 outbreak is Telemedicine. The progress of Hybrid/Decentralized clinical trials is streamlined through Telemedicine. Data indicates that shares of the company Zoom are up more than 150 % since the start of 2020 and shares of Microsoft [Which owns skype] are up more than 14% since the start of 2020. Some of this increase might also be due to the increase in remote working due to COVID, but it is likely some is due to Telemedicine.
Telemedicine not only reduces costs, but also time. For instance, it is estimated that on average, a person takes almost 2 Hours for an in-person physician/doctor visit2. Breaking down this 2 Hours:
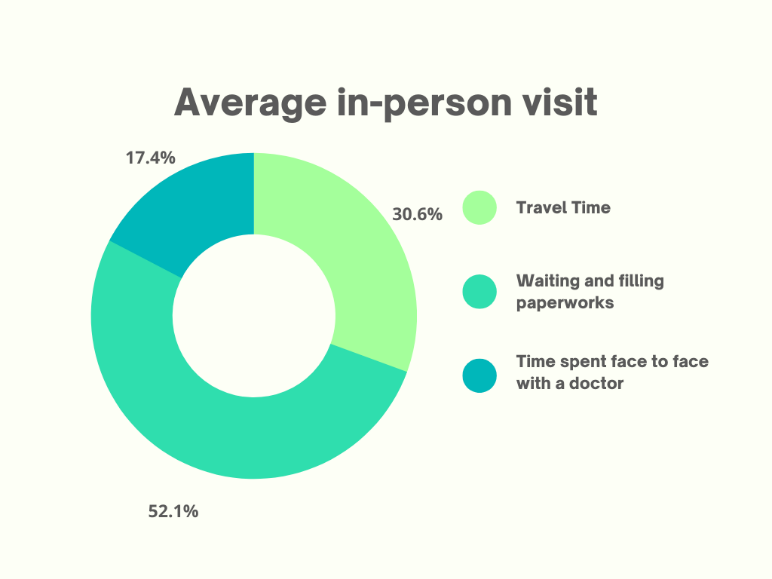
According to a study conducted by CISCO, over 74% of patients favour simple remote access to medical care services over in-person interactions3. An important factor when we consider any clinical trial is that it should be delivered in a patient- centric fashion. From the patient's point of view, it is way better in terms of cost and time not having to take a 2 -3 hour break from work for a doctor’s appointment.
Plus, patients don't have to invest a lot of time waiting, and for all the procedures associated with an in-person visit.
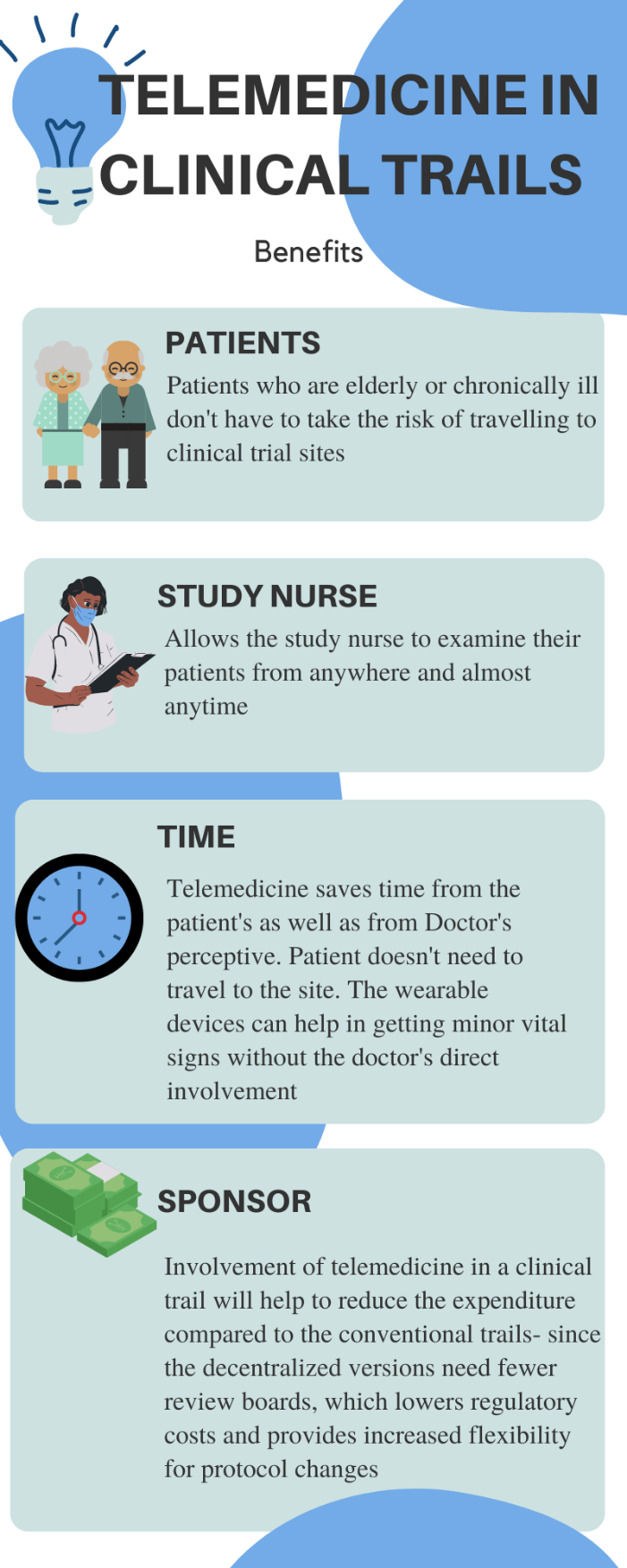
BENEFITS
Upon close examination, there are clear benefits of using Telemedicine in clinical trials for all stakeholders - shown by the infographic.
Future of Telemedicine
Artificial intelligence
AI powered technologies can serve as an anchor in automatic interactions with patients.
AI-based healthcare systems could detect symptoms and give information on medications, treatment, appointments etc., and there are many examples of these “monitoring” type applications in the news.
AI supported systems could also potentially improve the speed, accuracy, and precision of the process.
FDA approved the first AI based diagnostic device – which uses a self-optimizing algorithm based on deep learning to diagnose diabetic retinopathy. This algorithm enables a neural network to learn and execute a particular task through repetition and self-correction.
It is reported that this algorithm was trained with almost 0.12 million high-quality human-graded fundus images, which helped it to correct and learn how to diagnose diabetic retinopathy.
What's fascinating is the doctor's words on this technology –
Virtual reality / Augmented reality
Along with AI, VR/AR is also aiding in educating and training health care professionals and planning medical procedures. For visits, patients see and talk to their doctors as if they are standing nearby. Because, at the end of the day, humans are humans, and we need to interact with each other. The kind of engagement that happens when interaction happens face-to-face is entirely different to the remote version. In a clinical trial where everything is decentralized, VR/AR can aid with this “engagement” to an extent.
Conclusion
It’s no doubt that Telemedicine is here, adding value and being used but, still a few concerns exist.
The fundamental necessity of Telemedicine is the internet. In a recent survey done by Statista, more than 50 % of Indians don’t have access to internet4. And, even with internet access, bandwidth issues typically cause problems in video calls/consultations.
From a clinical trial point of view, patients need a proper private place to communicate with their doctors, lack of this will undoubtably affect the trial.
Even though Telemedicine allows doctors to examine their patients without the constraints of time and place, face-to-face interaction is always different. A physical touch, an eye-to-eye conversation aids in improving the mood of the patient and helps with diagnosis - which cannot be substituted by any technology.
However, it is highly likely that these hurdles with current Telemedicine will be overcome for the betterment of human health and the clinical trials industry.
If you would like to talk to us about this topic – please email us at info@zifornd.com
References